
Hi everyone! I visited BIOKOREA 2026 exhibition as a visitor few months ago, and I found one hot topic among all the biotech companies which even running out of brochures. It was ADC (surprisingly, not ABC). What is ADC? and why ADC is so popular amongst current biotech companies?
What does ADC stands for?
First of all, ADC is the abbreviation of Antibody Drug Conjugate. It's the new mechanism of anticancer treatment which utilises antibody - antigen relationships, specifically targeting the cancer cells. To understand this mechanism, you need to know what is antibody, antigen, and finally 'immune system' of our body.
Let's break down immune system
I assume most of you reading this article are already experts in this field. However, for those who might find these concepts a bit confusing, I’d like to give a super quick and easy overview of the immune system.
To put it simply, think of the immune system as a solid wall protecting our body from outside attackers!
Generally, our body operates two types of immune systems: innate immunity and adaptive immunity. Their initial responses to unverified substances are actually quite similar. I always use the metaphor of a company ID card when explaining this to non-major students. You’ve probably seen large corporate buildings that require an ID card for entry, right? Similarly, our body has a security gate to verify whether whatever enters is safe or not.
When our body spots an unverified substance at the gate, the security guards sound the alarm and activate the innate immune system. It’s like them saying, "Hey, your ID isn't in our system. Please leave the premises." The most common phenomenon triggered by this innate system is the inflammatory response. Our body deploys cells called macrophages to digest foreign substances. To help these cells move around more easily, our blood vessels widen, which is why a cut or wound turns red and swollen.
The Adaptive Immune System (Antigens & Antibodies)
However, some intruders cannot be dealt with by this initial guard response alone. In such cases, we need more detailed clues to uncover their identity. Think of it like a crime scene investigation where police look for fingerprints, dental records, or DNA to identify a suspect. It’s very similar in our bodies: these unverified substances carry their own unique 'fingerprints' called antigens. Helper T cells collect this antigen data and pass it along to B cells or Killer T cells, which then manufacture the specific weapons needed to eliminate the threat.
One of these primary weapons is the antibody, which is produced by B cells. The reason we get a flu shot almost every year is to update our immune system's 'recipe book' on how to create these weapons. That way, whenever the influenza virus enters, we can instantly recognize its antigen, open the recipe book, and mass-produce the necessary antibodies much faster.
As you can see, our body relies on a highly sophisticated immune system that is absolutely crucial to our survival. In fact, notorious diseases like AIDS are caused by a compromised immune system. On the flip side, if the immune system mistakenly attacks our own healthy cells, it leads to autoimmune diseases like lupus.
Another breakdown: cancer cells
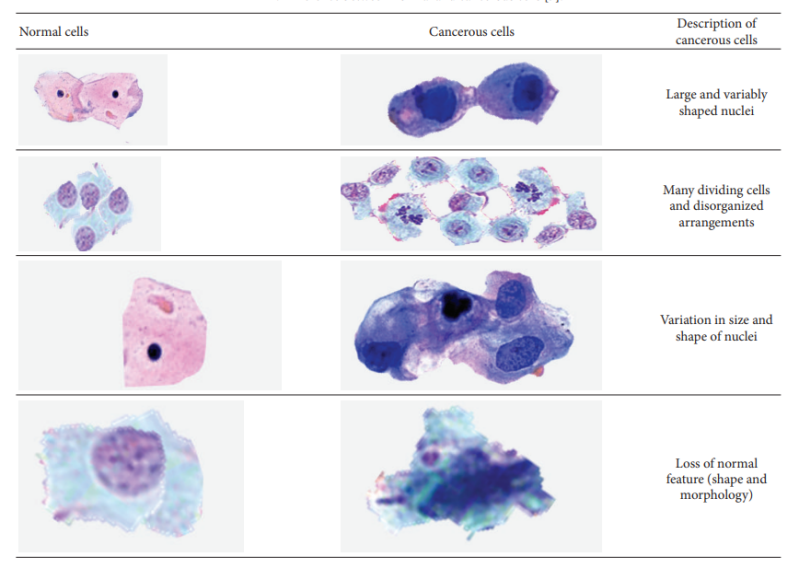
Table 1. Difference between normal and cancerous cells (Kumar et al., 2015)
Before we dive into ADCs, let’s get the basics down: What actually is a cancer cell?
Back in cancer biology class, the first word I learned was tumor. And honestly, tumors form a lot easier than you’d think. When the tightly regulated steps of cell division completely lose their brakes, cells start piling up into a lump. That lump is a tumor. If this cell cluster stays put and doesn’t spread, it’s called a benign tumor. But if it has the nasty habit of spreading (metastasis), it’s classified as a malignant tumor.
Given how terrifying the word 'cancer' sounds, these abnormal cells actually pop up in our bodies way more often and easily than we realize. The only reason it’s incredibly rare for cancer to actually take over is because our immune system is usually quick to attack and wipe them out. But as we age, our immunity naturally weakens. Our bodies can’t fight them off as effectively, and the cancer cells start winning the battle. This is exactly why the number of elderly cancer patients is much higher than younger ones.
The Big Three of Cancer Treatment: Chemo, Targeted, and Immunotherapy
According to the National Cancer Information Center, anticancer drugs are broadly categorised into three types: cytotoxic chemotherapy, targeted therapy, and immunotherapy.
1st Generation: Cytotoxic Chemotherapy
Cytotoxic chemo takes advantage of the fact that cancer cells divide incredibly fast, launching a direct attack on them. The downside? Because it's highly toxic, it also ends up attacking healthy, fast-growing cells in our body, leading to a lot of side effects. Instead of being used alone, it's usually paired with supportive treatments to help minimize those rough side effects.
2nd Generation: Targeted Therapy
Targeted therapy goes a step further than just looking at fast division. It zeroes in on the fact that cancer cells rely on specific protein signals to fuel their growth. By tracking these unique signals, it hunts down the cancer cells and blocks the pathways they need to grow and survive. Compared to the 1st generation, it's way more precise at sniping the actual target.
3rd Generation: Immunotherapy
As I mentioned earlier, our immune response is a massive deal in fighting cancer. When cancer cells suddenly crash the party in our body, they create new, unfamiliar proteins. Our body flags these proteins as foreign invaders and flips on the immune switch to attack the tumor. But cancer cells aren't stupid. They want to protect their clones, so they work hard to manipulate our immune system into leaving them alone. Immunotherapy figures out this sneaky tactic and turns our body's anti-tumor immune response all the way up to max, letting our own immune system wipe out the cancer.
Next generation anticancer treatment: ADC?
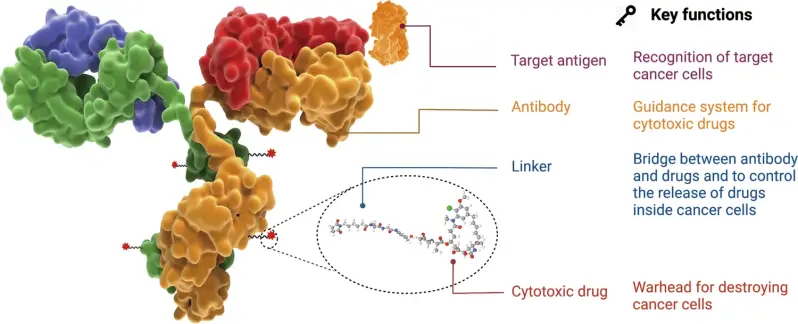
Fig 1. The structure and characteristic of an ADC drug (Fu et al., 2022)

Fig 2. How is ENHERTU thought to work? (Daiichi Sankyo, Inc, 2025)
As I mentioned earlier regarding the immune response, our bodies have specific antibodies that react only to specific antigens. They share a "Lock-and-key" structure where they fit together perfectly, meaning the antibody binds exactly to its specific target and nowhere else.
ADC (Antibody-Drug Conjugate) is a treatment method born right out of this highly specific antigen-antibody bond. Basically, scientists take an antibody that targets a specific antigen on a cancer cell, and hitch a ride on it with a powerful anticancer drug (called the payload). When this antibody latches onto the cancer cell's antigen, the linker connecting the antibody and the drug breaks, releasing the payload so it can do its job directly inside the cancer cell. Because it snipes the target with such insane precision, it’s currently getting massive attention and popularity as the next generation of cancer treatment.
Still a long journey to go...
Then.. does that mean ADCs are perfectly prepared for us and everything's ready?
I do have clear answer for this; the answer is no. Successfully developing an ADC is no walk in the park. There are so many variables to consider, making it a pretty tricky business. Every single piece of the puzzle, the antigen, antibody, linker, payload, and the conjugation technology used to stitch them together, has to fall perfectly into place to minimize side effects and maximize efficacy. Even the linker, which might seem like a minor detail, has to be stable enough to hold the drug and antibody together while surviving the bumpy ride through the bloodstream. On top of that, if the payload is too toxic, any accidental leak into the blood could cause severe side effects in healthy cells. Even the exact position where the drug is attached can drastically change the outcome. So yeah, it’s a pretty complex and sensitive little creature!
Let's breakdown the challenges
Given that ADCs have been researched more than decades now. you might wonder what have been the critical challenges, and how are we trying to cope with them? Let's break them down.
1: DAR
The biggest challenge with ADCs is achieving a high and uniform DAR (Drug-to-Antibody Ratio), which refers to the number of drugs attached to a single antibody. For instance, if some cannons carry only one bomb, others carry multiple, and some carry none at all, it would be impossible to achieve a precise and uniform anticancer effect. Initially, drugs were randomly conjugated to antibodies. This randomness led to early ADCs having very low efficacy or causing severe side effects that killed normal cells, ultimately leading to their withdrawal from the market.
2. Bystander Effect
Over time, next-generation ADCs with higher stability, such as Enhertu, have been developed, but they are still not perfect. Although Enhertu maintains a very high average DAR of 8, a 'bystander effect' has been observed, where the payload leaks into surrounding tissues and affects normal cells.
3. Eliminated & Various target proteins
Furthermore, while ADCs are highly effective against a single target, cancer cells can eliminate target proteins over time. Alternatively, targets may vary among cells within the cancer tissue, leaving the drug unable to find its way. There are still many hurdles to overcome, such as how to precisely control drug hydrophobicity, where to attach the drugs, and how many to attach.
Conclusion
Despite these tricky challenges, the global community is pouring immense capital and manpower into ADC development. This is because of the firm belief that the antigen-antibody mechanism of ADCs will open a new horizon in cancer therapy. Following previous mechanisms such as directly attacking cancer cells (cytotoxic chemotherapy), blocking substances secreted by cancer cells (targeted therapy), and enhancing anti-tumor immune responses (immunotherapy)—ADCs introduce a completely new concept that further enhances cell specificity through antigen-antibody reactions. They are highly anticipated to overcome chronic issues of existing therapies, such as side effects and drug resistance from long-term use, leading to more effective cancer treatments.
Personally, I am incredibly excited to see how cancer treatment evolves over the coming decades, and how humanity continues to tackle cancer—perhaps one of the greatest challenges in human physiology and medical science. What groundbreaking ADC therapies will global biotech companies unveil next?
Bibliography
Banner Image: Unsplash National Cancer Institute
Kumar, R., Srivastava, R., & Srivastava, S. (2015). Detection and Classification of Cancer from Microscopic Biopsy Images Using Clinically Significant and Biologically Interpretable Features. Journal of Medical Engineering, 2015, 1–14. https://doi.org/10.1155/2015/457906
Daiichi Sankyo, Inc. (2025). About ENHERTU | ENHERTU® (fam-trastuzumab deruxtecan-nxki) | HER2+ mBC. ENHERTU® (Fam-Trastuzumab Deruxtecan-Nxki) Patient Site. https://www.enhertu.com/en/breast/about-enhertu
Fu, Z., Li, S., Han, S., Shi, C., & Zhang, Y. (2022). Antibody drug conjugate: the “biological missile” for targeted cancer therapy. Signal Transduction and Targeted Therapy, 7(1). https://doi.org/10.1038/s41392-022-00947-7
National Cancer Institute. (2025, May 15). Types of Cancer Treatment. National Cancer Institute. https://www.cancer.gov/about-cancer/treatment/types
National Cancer Institute. (2022). Chemotherapy. National Cancer Institute; National Cancer Institute. https://www.cancer.gov/about-cancer/treatment/types/chemotherapy
National Cancer Institute. (2019, September 24). Immunotherapy to Treat Cancer. National Cancer Institute; Cancer.gov. https://www.cancer.gov/about-cancer/treatment/types/immunotherapy
Add comment
Comments